
Lung Cancer and Chest Disease Team
At Stony Brook Cancer Center, we know cancer affects every part of life. That’s why our Lung Cancer and Chest Disease Center offers personalized, expert care for lung cancer and other lung conditions. Our team diagnoses lung cancer at any stage and provides optimal care for other lung and chest diseases.
Members of the team include surgeons, medical oncologists, radiation oncologists and nurse practitioners. Additional specialists include radiologists, pathologists and the nursing staff. All of our health providers can easily collaborate and coordinate care because they are all right here at Stony Brook.
Is there a clinical trial right for you?
(631) 728-7425
Types of Lung Cancer and Chest Disease
Learn more about lung cancers and lung and chest diseases by clicking the links below:
- Non-Small Cell Lung Cancer
- Adenocarcinoma
- Squamous Cell Carcinoma
- Large Cell Undifferentiated Carcinoma
- Small Cell Lung Cancer
- Pulmonary Neuroendocrine Tumors
- Pulmonary Carcinoid Tumors
- Abnormal Chest CT findings (excluding lung nodules)
- Bronchopleural fistula (post-surgical): An abnormal passageway (a sinus tract) that develops between the large airways in the lungs (the bronchi) and the space between the membranes that line the lungs (the pleural cavity).
- Interstitial lung diseases: A large group of diseases that cause scarring, or fibrosis, of the lungs.
- Foreign body removal
- Lung nodules
- MAI (Mycobacterium avium-intracellulare) infection: Atypical mycobacterial infection.
- Mediastinal mass: Growths that form in the area of the chest that separates the lungs.
- Pleural effusion: A build-up of excess fluid between the layers of the pleura outside the lungs.
- Thymomas: A tumor (benign or malignant) originating from the epithelial cells of the thymus (a lymphoid organ in the neck that produces T cells for the immune system).
- Tracheal stenosis: A narrowing of the trachea, or windpipe, due to scar tissue formation or malformation of the cartilage in the trachea.
- Tracheobronchial malacia: When the walls of the airway (specifically the trachea and bronchi) are weakened, causing the airway to become narrow or collapse.
- Tracheoesophageal fistulas: An abnormal connection between the esophagus and trachea (windpipe).
Lung Cancer Screening Program
Finding lung cancer early can improve survival rates to as high as 90 percent. Our Lung Cancer Screening and Prevention Program offers annual low-dose CT scans for individuals at high risk. Each case is reviewed by our expert team of lung cancer specialists, following U.S. Preventive Services Task Force guidelines. If treatment is needed, you’ll have access to Stony Brook’s nationally recognized Lung Cancer and Chest Disease Program, where specialists provide personalized care.
According to the U.S. Preventive Services Task Force, if you are between the ages of 50 and 80 and have a smoking history of 20 years or more, or currently smoke, or quit within 15 years, you should consider getting a low-dose CT scan.
Other factors that may put you at risk are exposures to:
- Toxins through a job
- Second-hand smoke
- Harmful toxins through military service
- World Trade Center dust or other hazardous materials
The Lung Cancer Screening and Prevention Program has screened hundreds of patients. Lung cancer has been found in a small percentage of individuals. All were found at an early, curable stage. More than 40 percent of our participants are current smokers and have received counseling for tobacco cessation. Many have been able to reduce the amount they smoke or have completely quit smoking.
For an appointment with our Lung Cancer Screening and Prevention Program, call (631) 638-7000.
Our Lung Cancer and Chest Disease Team
Surgery

Medical Oncology


Radiation Oncology

Interventional Pulmonology

Interventional Radiology

Diagnosing Lung Cancer
The multidisciplinary Lung Cancer and Chest Disease Management Team creates an optimal treatment plan based on the individual’s needs. The specialists on the team include cardiothoracic surgeons, interventional pulmonologists, medical oncologists, radiation oncologists, interventional radiologists, pathologists, oncology-certified nurse practitioners and nurses. A meeting is held once a week where the specialists discuss, coordinate and collaborate on each patient’s treatment plan.
Several diagnostic tests may be ordered to evaluate whether you have lung cancer and what stage (definition) it is. Doctors may also order tests to evaluate the condition of your lungs and/or heart.
Diagnostic Tests for Lung Cancer
The following are some commonly ordered tests:
- Chest X-Ray: A chest x-ray (CXR) is an x-ray image of the chest, lungs, heart, large arteries, ribs and diaphragm. It looks like the negative of a photograph. This test is performed in our hospital's radiology department. Two views are usually taken: one in which the x-rays pass through the chest from the back (posterior-anterior view), and one in which the x-rays pass through the chest from one side to the other (lateral view). You stand in front of the x-ray machine and must hold your breath when the x-ray is taken.
- CT Scan: Computed tomography, also called computerized axial tomography (CAT), is an x-ray imaging technique that produces pictures of slices or cross-sections through the body. It is used to tell the size of a tumor, whether the lymph nodes are enlarged, or whether other organs of the body are affected.
- MRI: Magnetic resonance imaging uses a strong magnet and radio waves to make images of the body. It is often useful to see if cancer has spread (metastasized) to the brain.
- PET Scan: Positron emission tomography is an imaging technique in which a form of sugar with a radioactive tracer is injected into the patient, and then a special camera takes pictures. Cells that are highly metabolic, such as cancer cells, take up this sugar and show up as "hot spots." These images are useful in providing an indication of whether the tumor is cancerous or whether the lymph nodes are involved.
- Pulmonary Function Test: This test (also known as PFT) is a breathing test that measures how well your lungs are working.
- Cardio-Pulmonary Exercise Test: This test (also known as CPET) is performed to evaluate your lung function in relationship to your heart.
- Cardiac Stress Test: This test is performed to evaluate the condition of your heart. You may be asked to do the form of the test in which you run on a treadmill; or the form in which a medication is given to you through an IV line (intra-venous; into a vein), after which special x-rays are often taken of your heart.
A biopsy refers to the removal and examination of tissue and cells from a tumor or lymph node. This test is used to help make a diagnosis of lung cancer, as well as to determine the "stage" of a possible cancer. The sample of tissue or cells taken for a biopsy is sent to the pathologist who evaluates it.
Biopsy Techniques for Lung Cancer
The following techniques are used:
- Bronchoscopy: A pulmonologist (lung specialist) uses an endoscope (a device that consists of a tube and an optical system) to look down your bronchus and take tissue samples.
- Mediastinoscopy: A surgeon makes a small incision just above your breastbone and uses a scope to look under your breastbone to take tissue samples.
- Thoracoscopy: A surgeon makes three small incisions on the side of your chest between your ribs and uses a scope to look at the lung and pleural spaces. Tissue samples are then taken. This kind of procedure requires a stay in the hospital.
- Fine-Needle Aspiration: A very thin needle attached to a syringe is inserted into a tumor to withdraw a small amount of cells. Many times an ultrasound or CT scan is used to help guide the needle to penetrate the tumor.
Stony Brook Cancer Center’s Lung Nodule Program is part of the overall comprehensive Lung Cancer and Chest Disease Center. The focus of this program is diagnosing and managing
pulmonary nodules to ensure proper surveillance for early detection of lung cancer. A nodule is a small mass of tissue in the lung. Most lung nodules are noncancerous (benign).
The most common causes of developing lung nodules include:
- Clumps of inflamed tissue due to an infection or inflammation (granulomas)
- Benign lung tumors (hamartomas)
- Infections such as TB/fungal infections
- Sarcoidosis
The most common causes of malignant lung nodules include lung cancer or cancers from other
regions of the body that have spread to the lungs (metastatic cancer). The larger the nodule the
more likely the risk of malignancy. In this case, further testing is warranted.
Most patients with lung nodules have no symptoms at all. A patient’s symptoms may include:
- Dyspnea (shortness of breath)
- Weight loss
- Hemoptysis (coughing up blood)
- Cough
The majority of lung nodules are found incidentally during a routine visit or by being evaluated for other medical issues. Many times, when a CT scan of the abdomen is performed, the base of the lung is visible and nodules are found. At other times, a nodule on a chest x-ray may be discovered during pre-testing for a procedure. In this case, a dedicated CT scan of the chest is recommended. A patient’s primary care doctor or a specialist can provide a referral to the Lung Nodule Program.
Interventional pulmonologists can diagnose, stage and treat conditions and cancer of the lungs. They are part of the comprehensive lung cancer program at Stony Brook Cancer Center.
Staging is an important part of cancer diagnosis because it is a common language that all healthcare providers understand and is used to assess the extent of the disease.
Treatment and Care
We create a personalized care plan for each patient, considering their age, overall health and the cancer’s type, size, location and stage. Before surgery, we assess lung function to determine how much tissue can be safely removed and how well the patient will function afterward.
The goal of surgery is to remove the cancerous part of the lung and nearby lymph nodes, which are examined to check for cancer spread.
How Surgery is Performed:
- Robotic-assisted surgery: A minimally invasive procedure that highly trained surgeons perform with the da Vinci® Xi™ robotic system for a lobectomy. The surgeon docks the robotic console right next to the patient and uses this tool as an extension of their hands and magnification of their vision. Learn more about robotic-assisted surgery for lung cancer.
- Thoracoscopy or VATS (video-assisted thoracic surgery): Removal of the tumor and surrounding lymph nodes by a minimally invasive thoracic surgery in which a tiny camera (thoracoscope) and surgical instruments are inserted into the patient’s chest through one or more small incisions in the chest wall.
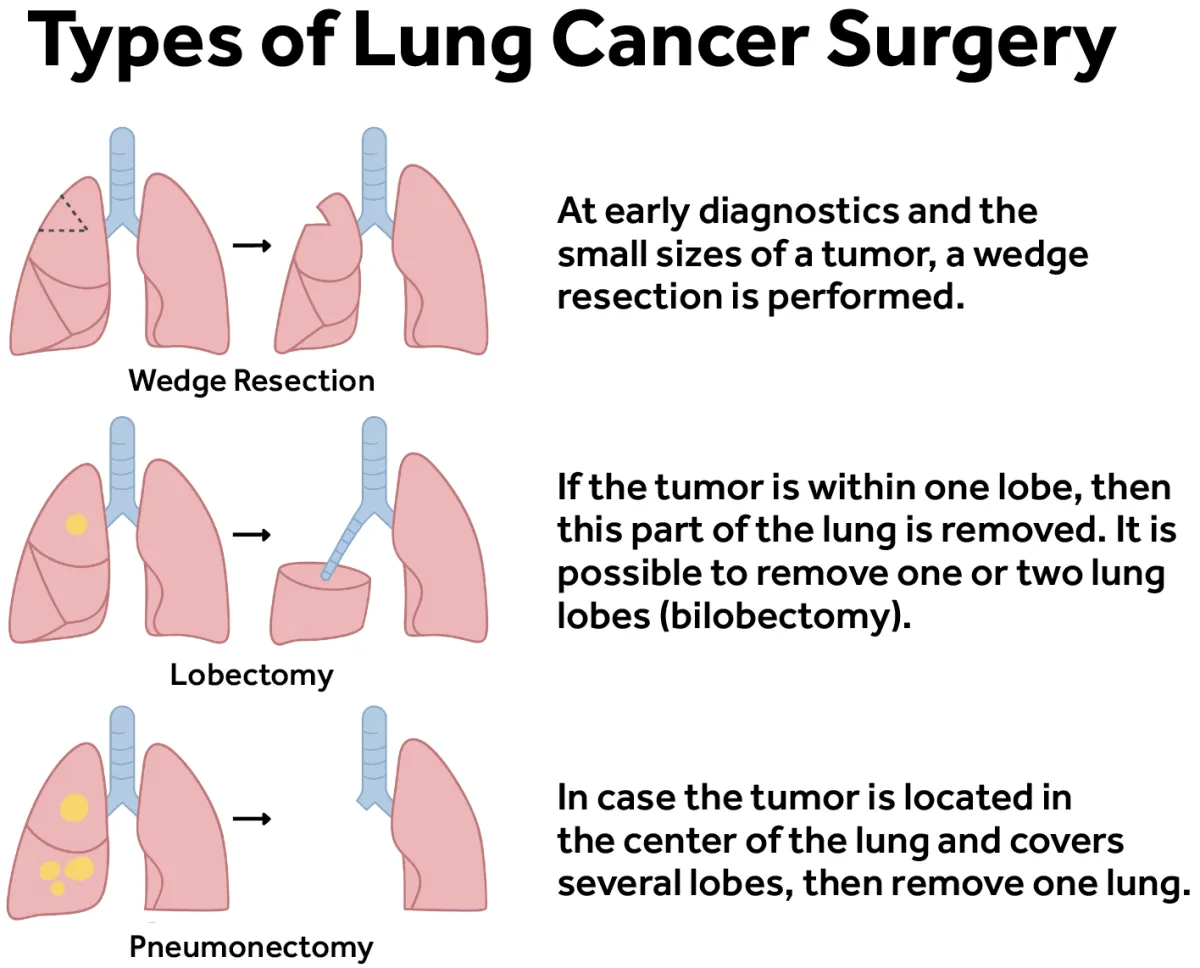
Types of Surgery:
- Wedge resection-removal: Removal of the tumor and the part of the surrounding lung in the shape of a piece of pie (wedge). This procedure is performed to obtain a biopsy. The tissue can be sent to the pathologist for examination while the patient is still in surgery. If the pathologist determines that it contains cancer, the surgeon then performs a lobectomy. A surgeon may recommend this procedure for a patient who cannot tolerate a lobectomy.
- Segmentectomy or segmental resection: Removal of part of the lobe where the cancer is located. The segmentectomy is typically performed on patients who have limited lung capacity and can’t tolerate the removal of a larger section of the lung. This is also a good option for patients with small early-stage tumors (measuring less than two centimeters).
- Lobectomy: Removal of the lung lobe containing the cancer with the goal to cure lung cancer. The lobectomy is considered the gold standard for lung cancer treatment.
- Pneumonectomy: Removal of the entire lung, usually because the tumor is centrally located.
Medical oncologists play a key role in treating lung cancer as part of a multidisciplinary team at Stony Brook Cancer Center. They work closely with surgeons, radiation oncologists and other specialists to create personalized treatment plans.
After reviewing a patient’s medical history and diagnosis, the medical oncologist determines the best treatment approach, which may include chemotherapy, oral medications or immunotherapy.
Chemotherapy for Lung Cancer
Chemotherapy uses drugs to destroy cancer cells, either by mouth, injection or through an IV. These drugs target dividing cells, aiming to kill cancer cells, which divide more rapidly than normal cells. However, some normal cells may also be affected, leading to side effects.
- How Chemotherapy Works: Chemotherapy is given in cycles, allowing normal cells time to recover between treatments. The number and timing of cycles depend on the type and stage of cancer and the specific drug used.
- Side Effects: Common side effects include nausea, fatigue, hair loss, mouth sores and infections. Many of these improve after treatment ends. Medical oncologists work closely with patients to manage and minimize side effects.
- Before or After Surgery: Chemotherapy may be used before surgery (neo-adjuvant) to shrink tumors or after surgery (adjuvant) to eliminate remaining cancer cells, enhancing the effectiveness of surgery.
Thanks to advancements in treatment, modern chemotherapy is more tolerable and most patients experience fewer severe side effects compared to the past.
Immunotherapy for Lung Cancer
This treatment boosts the immune system to fight cancer using proteins derived from living cells. These are injected to ensure effectiveness, as they cannot be taken orally.
The team meets regularly to collaborate on each patient’s care, ensuring the best possible outcomes.
Radiation oncology is a medical specialty that in many cases can be the single most effective method to treat lung cancer. It may also be combined with surgery and/or chemotherapy to help increase its effectiveness.
Radiation therapy is a safe and effective use of high-energy x-rays to kill or shrink cancer cells, while preserving the normal, surrounding tissue. It’s often an option for someone who has early stage lung cancer, as well as for more advanced cancers. In the case where cancer has spread, radiation therapy can also help to relieve symptoms.
Radiation oncology offers different modalities of treatment:
Interventional radiology is a medical specialty that uses imaging to guide minimally invasive procedures. These techniques involve tiny incisions and are used for both diagnosis and treatment. Compared to traditional surgery, they cause less pain and have shorter recovery times. The doctors who perform these procedures are called interventional radiologists.
Interventional radiologists use the following imaging techniques:
- CT scans
- Ultrasound
- Fluoroscopy
- MRI (occasionally)
How Does Interventional Radiology Treat Lung Cancer?
While surgery is the preferred treatment for early-stage lung cancer, some patients may not be candidates for traditional surgery due to health or lung conditions. For these patients, interventional radiology offers minimally invasive options like thermal ablation to destroy cancer cells.
Types of Thermal Ablation
- Cryoablation: Uses extreme cold to destroy cancer cells.
- Microwave or Radiofrequency Ablation: Uses heat energy to target cancer cells.
How It Works
- Needles are placed in or around the lung tumor using CT imaging for guidance.
- Energy (heat or cold) is delivered through the needles to destroy the cancer cells.
- The procedure is done under general anesthesia, with most patients staying overnight for observation and going home the next day.
Follow-Up Care
After treatment, you’ll have regular follow-ups with CT and PET scans to monitor progress. If the cancer returns or the tumor doesn’t fully respond, the procedure can be repeated.
Information For Patients
To make an appointment, please call (631) 444-2981. Our fax number is (631) 444-6970.
Please read the information below and gather as much of what's listed together before you call. If you do not have something on the list or you have a question, call us and we can guide you through what you need.
We will need the following information (if you have it available at the time of your call, that would be very helpful):
- Your name and contact information (home phone, cell phone, home address)
- Insurance information
- The reason you are being referred to us
You will need to have had a recent CT (computed tomography) scan of your chest, and have the report faxed to us. If you have not had a CT scan yet, call us and we can assist you with your next step to make that appointment. If your CT scan was not performed at Stony Brook University Hospital, please bring a copy of your CT scan (either the films or a CD) to your first appointment with us. Without access to the images, we will not be able to provide a full evaluation.
We would like to have copies of the following test reports:
- Recent blood work
- Breathing test
- Stress test
- Biopsy (pathology report)
We will also need information about:
- Your past medical and surgical history
- What medications you take
- Any allergies you may have
Survivorship Program for Patients with Lung Cancer
At Stony Brook Cancer Center, survivorship begins the day of diagnosis and continues through the end of treatment. Our Survivorship Program focuses on reducing the risk of lung cancer recurrence and supporting patients as they transition to life after treatment.
What to Expect:
- A 30-minute appointment with a certified nurse practitioner
- A personalized packet with:
- Diagnosis and treatment summary
- Five-year follow-up schedule
- Booklets on life after cancer, wellness and nutrition
- Support group and resource information
This appointment, typically scheduled 1–2 months after treatment ends, is an opportunity to address questions, concerns and focus on the future. Patients often find it uplifting and empowering.