
In the event of any unusual findings in your BSE, do not procrastinate; see your doctor immediately for a definite diagnosis. Above all, do not abandon your BSE after several "normal" inspections. BSE cannot protect you if you don't use it.
The following describe three differnt approaches:
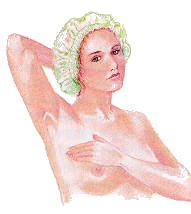
Lying Down
Begin while lying in bed. Place a pillow or folded town under your left shoulder and your left hand behind your head. Your shoulder should be raised high enough for your left breast to be center on top of your chest, falling neither to the center nor toward the armpit; this arrangement distributes the breast tissue as evenly as possible across the chest 
wall. If a breast is not properly flattened against the chest, it is difficult to feel a lump – particularly in the outer upper quadrant, where tissue is thickest (and where most malignancies occur).
Palpation, a careful and systematic feeling of your breasts, will give you a "touch picture" of their normal structure and condition. Also use your right hand to examine your left breast, and vice-versa. Use two or three fingers, keeping the thumb extended, and always feel with the sensitive "palmar pads" on the flat, inner surfaces of your fingers. Do not use fingertips as they are less sensitive, and long fingernails will impede you examination. Never compress your breast between thumb and fingers as this may cause you to feel a "lump" that doesn’t exist.
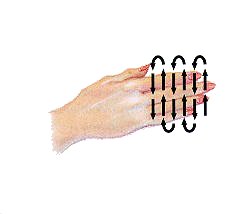
Be thorough. Examine the entire are, including the lymph nodes, from your collarbone to just below your breasts, and from armpits to breastbone.
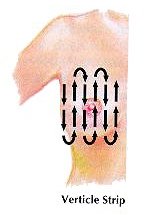
The National Cancer Institute developed the vertical or linear method of breast self examination. This method is now recommended by the American Cancer Society. Recent research suggests this up and down pattern of BSE is more thoroughly followed by many women. What is most important is that the entire breast, with special attention focused on the area between the breast and underarm area itself, be included in the examination.
When examining your breast using this vertical method, start in the underarm area and have your fingers move downward little by little until you reach the area below the breast. Then move your fingers slightly toward the middle and slowly move back up. Go up and down until the entire area is covered.
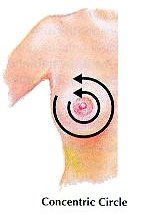
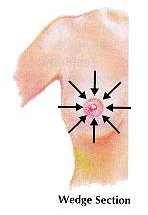
Some women feel more comfortable using the circular method of BSE while others may divide the breast into wedges, covering one small wedge section at a time. What is most important in whatever method you use is that the underarm and upper chest areas be examined as well as the entire breast area. When examining your breasts, press gently but firmly to immobilize the skin and roll fingertips over the underlying tissue. Merely sliding the fingertips over the skin does not tell you anything about conditions below the surface. Go over each area three times using (1) light, (2) medium and (3) firm pressure.
When you have finished examining your left breast with your left arm under your head, repeat the entire examination with your left arm in a relaxed position at your side. (Remember to keep your fingers flat.)
Next, shift the pillow to your right side; examine your right breast with your left hand, in both the arm-overhead and arm-at-your-side positions.
Carefully notice the "feel" of your normal breast structure, so that you can note at once any changes from what is usual for you. Many women have a normal thickening or ridge of firm tissue under the lower curve of the breast, at its attachment to the chest wall; also the large milk ducts can be felt as a ring of bumps. At the outer edge of the areola. In very slender women, the bony prominences of the chest wall my be mistaken for chest tumors, as may enlarged milk glands, fat tumors, lymph nodes, or benign cysts. All such thickenings should be palpated carefully during each monthly BSE, in order to distinguish stable, normal conditions from potentially dangerous changes. Any lump or other change found in one breast only (especially in the upper outer quadrant) is more likely to be serious than a change which has a mirror image in the other breast. If in doubt about ANY development, consult your doctor.
In the Shower
 Many lumps are more easily felt when breast and fingers are wet and slippery with soap lather (it reduces the friction). If your breasts are small, place one hand on your head and examine the breast on the side with your opposite had in an up-and-down pattern, as you do lying in bed. If your breasts are large or pendulous, you will be better able to feel them if you immobilize a breast with one hand (first supporting from below, then pressing down from above) and examine it with the other hand (first from above, and then from below).
Many lumps are more easily felt when breast and fingers are wet and slippery with soap lather (it reduces the friction). If your breasts are small, place one hand on your head and examine the breast on the side with your opposite had in an up-and-down pattern, as you do lying in bed. If your breasts are large or pendulous, you will be better able to feel them if you immobilize a breast with one hand (first supporting from below, then pressing down from above) and examine it with the other hand (first from above, and then from below).
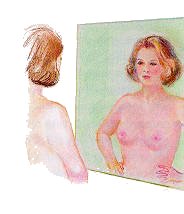
In the Mirror
Some breast disorders will reveal themselves by changes obvious to visual inspection. Again, it is important to become familiar with the normal appearance of your breasts, no woman has two exactly identical breast; many women’s breasts are markedly dissimilar. What is important in visual BSE is not the normal difference between your two breasts, but any change in one breast without a similar change in the other.
 |
 |
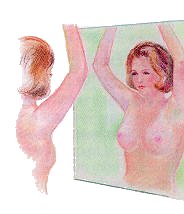
With your upper body unclothed, stand in front of a large mirror; a good light should be placed off to one side, rather than directly above the mirror or overhead – side lighting helps show irregularities.
Examine the appearance of your breasts (1) with arms relaxed at your sides; (2) with arms raised; (3) with hands clasped in front of the forehead, palms squeezed together, to tighten chest pectoral muscles; (palms flat on sides of hips, pressing down. In each of these positions, observe your breasts first directly facing the mirror, then while slowly turning from side to side.
Note the contours and relative placement of your breasts, the appearance of the areolae and nipples, any distortions or discolorations of the skin or surface texture and their movement as you move your arms and chest muscles. Consider any medical factors (injury, surgery, etc.) or activities (one-sided exercise, such as bowling, tennis, operating machinery, etc.) that might account for either differences or changes in symmetry.
Certain skin condition may signal danger to the breasts. Redness, irritation or prominent veins may indicate an increased blood supply that often accompanies tumor growth. Also look for whitish scale on the nipple or areolae, ulcers, sores or surface erosion that does not heal promptly; or any changes in a pigmented (black or brown) mole anywhere within the breast area. Blocked lymph ducts which may be associated with the growth of tumors can result in "orange-peel" skin – swollen and shiny with deep enlarged pores. Although all of these signs may also be connected with benign conditions, the presence of any of then should signal you see immediate medical attention.
Last inspect your nipples and areolae for changes in size, shape, color, or location; note any flattening, dimpling, indentation or retraction. Of special concern should be any change or distortion of the normal nipple, for distorted ligaments may "point" the nipple toward an adjacent malignant tumor. A flat, inverted or retracted nipple, if it is a recent development should also be regarded as a danger signal; likewise, a nipple which is inverted (outward-pointing) when you are upright but inverts when you lean forward.
There appears to be differences of opinion regarding "milking" or squeezing the nipples to determine if there is any nipple discharge. In the 1995 edition of the medical book, "Ambulatory Gynecology," edited by Drs. D. H. Nichols and R. L. Sweeney, it states, milking or squeezing is only recommended when there is a history of nipple discharge.
It is particularly important that your visual BSE include all the maneuvers detailed. The Cooper’s ligaments that determine and maintain breast structure are delicate and likely to be distorted by the growth of cancer tumors; these tumors adhere to the ligaments – or to the pectoral muscles, nipples, or skin -- and result in visible changes in breast contours. Such changes may appear as swelling or flattening, bulges, dimples, or retraction of any area not previously so affected. A fifth maneuver, bending forward from the hips with hands supported on knees or chair backs, allows the breasts to hang straight forward; this position most greatly accentuates both normal and abnormal variances. Normal breast structure falls away in the leaning forward position, and any cancerous entanglement of the Cooper’s ligaments will be revealed by a visible distortion in the area affected.